Contracted Toe Treatment
 Overview
Overview
There are two different types of Hammer toes. Flexible Hammer Toes. These hammer toes are less serious because they can be diagnosed and treated while still in the developmental stage. They are called flexible hammer toes because they are still moveable at the joint. Rigid Hammer Toes. This variety is more developed and more serious than the flexible condition. Rigid hammer toes can be seen in patients with severe arthritis, for example, or in patients who wait too long to seek professional treatment. The tendons in a rigid hammer toe have become tight, and the joint misaligned and immobile, making surgery the usual course of treatment.
Causes
Hammer toe is often caused by wearing shoes that do not fit properly. If shoes are too small either in length or width, then the toes are held in a shortened position for long periods and the muscles eventually shorten and pull the toes into the bent position. Alternatively it can be caused by overactivity in the extensor digitorum dongus muscle (right) and a weakness in the counteracting muscle under the foot, such as flexor digitorum longus. Sometimes it can be a congenital condition, meaning it is present from birth. It is also more common in those with arthritis in the foot or diabetes.
 Symptoms
Symptoms
If the toes remain in the hammertoe position for long periods, the tendons on the top of the foot will tighten over time because they are not stretched to their full length. Eventually, the tendons shorten enough that the toe stays bent, even when shoes are not being worn. The symptoms of hammertoe include a curling toe, pain or discomfort in the toes and ball of the foot or the front of the leg, especially when toes are stretched downward, thickening of the skin above or below the affected toe with the formation of corns or calluses, difficulty finding shoes that fit well. In its early stages, hammertoe is not obvious. Frequently, hammertoe does not cause any symptoms except for the claw-like toe shape.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits).
Non Surgical Treatment
You can usually use over-the-counter cushions, pads, or medications to treat bunions and corns. However, if they are painful or if they have caused your toes to become deformed, your doctor may opt to surgically remove them. If you have blisters on your toes, do not pop them. Popping blisters can cause pain and infection. Use over-the-counter creams and cushions to relieve pain and keep blisters from rubbing against the inside of your shoes. Gently stretching your toes can also help relieve pain and reposition the affected toe.
Surgical Hammer toes Treatment
Surgery is used when other types of treatment fail to relieve symptoms or for advanced cases of hammertoe. There are several types of surgeries to treat hammertoe. A small piece of bone may be removed from the joint (arthroplasty). The toe joint may be fused to straighten it (arthrodesis). Surgical hardware, such as a pin, may be used to hold the bones in place while they heal. Other types of surgery involve removing skin (wedging) or correcting muscles and tendons to balance the joint.
What Are The Principal Causes Of Hallux Valgus?
Overview
 A foot bunion is when the big toe gradually deviates inwards towards the second toe and in severe cases may even start to cross over the top or underneath. As the top of the toe moves inwards, the base of the toe (the knuckle part), pushes outwards producing the characteristic lump on outer side of the big toe. The medical term for a foot bunion at the big toe is a hallux abducto valgus, or hallux valgus. ?Hallux? means big toe, ?abducto? means to move away from the midline and ?valgus? refers to the abnormal angle of the toe. Foot bunions can also occur in the little toe, where they are known as a bunionette, but these are much less common.
A foot bunion is when the big toe gradually deviates inwards towards the second toe and in severe cases may even start to cross over the top or underneath. As the top of the toe moves inwards, the base of the toe (the knuckle part), pushes outwards producing the characteristic lump on outer side of the big toe. The medical term for a foot bunion at the big toe is a hallux abducto valgus, or hallux valgus. ?Hallux? means big toe, ?abducto? means to move away from the midline and ?valgus? refers to the abnormal angle of the toe. Foot bunions can also occur in the little toe, where they are known as a bunionette, but these are much less common.
Causes
Bunions result from the long bone in the foot (metatarsal) and the big-toe bone becoming misaligned. The causes are likely to be a combination of genetics, wearing ill-fitting shoes, and the way that we walk or run. Arthritis sufferers are also prone to bunions.
Symptoms
The symptoms of a bunion include the following development of a firm bump on the outside edge of the foot, at the base of the big toe, redness, swelling, or pain at or near the MTP joint, corns or other irritations caused by the overlap of the first and second toes, restricted or painful motion of the big toe.
Diagnosis
Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly.
Non Surgical Treatment
Sometimes observation of the bunion is all that's needed. A periodic office evaluation and x-ray examination can determine if your bunion deformity is advancing, thereby reducing your chance of irreversible damage to the joint. In many other cases however some type of treatment is needed. Early treatments are aimed at limiting the progression of the deformity and easing the pain of bunion or an associated joint. Conservative treatments such as orthotics can achieve this but they won't reverse the deformity itself. These options include changes in shoewear. Padding. Pads placed over the area of the bunion can help minimise pain, but will not stop the progression of the bunion. Activity modifications. Avoid activity that causes bunion pain, this could include standing for long periods of time. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may help to relieve pain. Icing. Applying an ice pack several times a day helps reduce inflammation and pain. Orthotic devices. Orthotics are the mainstay of non-surgical treatment for bunions. 
Surgical Treatment
Surgical options, such as a bunionectomy, can remove the bunion and realign the toe. There are several types of surgeries to fix the bunion. The type of bunion you have along with other factors such as the degree of severity and underlying cause of the bunion will determine which approach would be most beneficial for you.
Prevention
To minimize the chance of developing bunions, never force your feet into shoes that don?t fit. Choose a shoe that conforms to the shape of your foot. Opt for shoes with wider insteps, broad toes, and soft soles. Shoes that are short, tight, or sharply pointed should be avoided.
Do You Know The Primary Causes Of Overpronation Of The Foot
Overview
Pronation, in anatomical terms, means to rotate, and it applies to any rotational movement of a bone. Pronation in the feet involves an inward rolling of the foot throughout the gait which helps with the transfer of force. Normally the foot will move from the heel to the toes with only a small degree of pronation, with a slight inward roll from the outside of the heel to the inside of the foot which helps to support the body weight. Normal pronation involves the rolling of the foot to approximately 15 degrees. If you have normal foot arches, you are likely to be a neutral runner and will most likely pronate normally.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
Pronation, in anatomical terms, means to rotate, and it applies to any rotational movement of a bone. Pronation in the feet involves an inward rolling of the foot throughout the gait which helps with the transfer of force. Normally the foot will move from the heel to the toes with only a small degree of pronation, with a slight inward roll from the outside of the heel to the inside of the foot which helps to support the body weight. Normal pronation involves the rolling of the foot to approximately 15 degrees. If you have normal foot arches, you are likely to be a neutral runner and will most likely pronate normally.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
What Is Severs Disease?
Overview
Sever?s disease is a painful condition of the heel affecting children, usually at the beginning of the growth spurt in early puberty. It is caused by inflammation at the growth plate at the back of the heel, adjacent to the Achilles tendon attachment. This is one of the most common causes of heel pain in school-aged children. Physically active children aged between eight and fourteen years old are most at risk of developing pain from Sever?s disease. It is common among children involved in soccer, little athletics, gymnastics, basketball and netball but can affect children involved in any running or jumping activity. Boys seem to be more commonly affected than girls.
Causes
Contraction of the calf muscles along with the rapid growth of the leg bone (tibia), decreases ankle motion and increases strain on the heel area. This puts strain on the Achilles tendon. Injury results from repetitive pulling through the heel bone by the Achilles and the traction forces from the plantar fascia.
Symptoms
Symptoms include heel pain related to sports activities and worsen after those sport and exercise activities. However, some children who are not in a sport may also get this if they are physically active. If you notice that your child is ?walking on their toes? this is a sign of possible heel pain. The pain is usually on the back of the heel, the sides of the heel, the bottom of the heel, or a combination of all of these. We typically don't see swelling with this, however if pressure is applied to the sides of the heel pain may be reported. Sometimes the pain is so bad the child will have to limp, or take a break from sports activity either for a few days or few months.
Diagnosis
Sever's disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order X-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The treatment of Sever's disease should be individualized. The most important first steps in the treatment of Sever's disease are activity modification (including rest and sometimes crutches) and good shoes. Further treatment may include icing to decrease pain around the calcaneal apophysis, stretching and strengthening exercises, shoe orthotics or medications to relieve pain. Rarely, a removable cast is necessary to completely rest the foot.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Sever?s disease is a painful condition of the heel affecting children, usually at the beginning of the growth spurt in early puberty. It is caused by inflammation at the growth plate at the back of the heel, adjacent to the Achilles tendon attachment. This is one of the most common causes of heel pain in school-aged children. Physically active children aged between eight and fourteen years old are most at risk of developing pain from Sever?s disease. It is common among children involved in soccer, little athletics, gymnastics, basketball and netball but can affect children involved in any running or jumping activity. Boys seem to be more commonly affected than girls.
Causes
Contraction of the calf muscles along with the rapid growth of the leg bone (tibia), decreases ankle motion and increases strain on the heel area. This puts strain on the Achilles tendon. Injury results from repetitive pulling through the heel bone by the Achilles and the traction forces from the plantar fascia.
Symptoms
Symptoms include heel pain related to sports activities and worsen after those sport and exercise activities. However, some children who are not in a sport may also get this if they are physically active. If you notice that your child is ?walking on their toes? this is a sign of possible heel pain. The pain is usually on the back of the heel, the sides of the heel, the bottom of the heel, or a combination of all of these. We typically don't see swelling with this, however if pressure is applied to the sides of the heel pain may be reported. Sometimes the pain is so bad the child will have to limp, or take a break from sports activity either for a few days or few months.
Diagnosis
Sever's disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order X-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The treatment of Sever's disease should be individualized. The most important first steps in the treatment of Sever's disease are activity modification (including rest and sometimes crutches) and good shoes. Further treatment may include icing to decrease pain around the calcaneal apophysis, stretching and strengthening exercises, shoe orthotics or medications to relieve pain. Rarely, a removable cast is necessary to completely rest the foot.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Which Are The Key Causes Of Adult Aquired Flat Foot ?
Overview
Adult acquired flat foot was first described in the late 1960s as something that occurred after trauma, as a result of a tear to the tibial posterior tendon. However, by 1969 two doctors called Kettlekamp and Alexander described cases in which no trauma had taken place. They referred to the condition as "tibial posterior tendon dysfunction" and this became known as the most common type of adult acquired flat foot. 
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
Treatment of Adult Acquired Flatfoot Deformity depends on the stage of progression, as mentioned above paragraphs. Below we will outline a variety of different treatment options available. Orthotics or bracing. To give your foot the arch the support it needs, your podiatrist or foot specialist may provide you with over the counter brace or a custom orthotic device that fits your shoe. Casting. In some cases, a cast or boot is worn to stabilize the foot and to give the tendon time to heal. Physiotherapy. Ultrasound treatments and exercises may help rehab the tendon and muscles. Medications. Over-the-counter (NSAIDS) such as ibuprofen can help reduce pain, inflammation and swelling associated with AAFD. Shoe Gear. Your podiatrist may suggest changes with your shoes you are wearing and inserts you need in your shoe to help support your arch. 
Surgical Treatment
Although non-surgical treatments can successfully manage the symptoms, they do not correct the underlying problem. It can require a life-long commitment to wearing the brace during periods of increased pain or activity demands. This will lead a majority of patients to choose surgical correction of the deformity, through Reconstructive Surgery. All of the considerations that were extremely important during the evaluation stage become even more important when creating a surgical plan. Generally, a combination of procedures are utilized in the same setting, to allow full correction of the deformity. Many times, this can be performed as a same-day surgery, without need for an overnight hospital stay. However, one or two day hospital admissions can be utilized to help manage the post-operative pain. Although the recovery process can require a significant investment of time, the subsequent decades of improved function and activity level, as well as decreased pain, leads to a substantial return on your investment.
Adult Aquired FlatFoot (AAF) The Small Print
Overview
Have you noticed the arch in your foot collapse over a fairly short period of time as an adult? Or Do you suffer from pain on the inside and sole of your arch? If it does, then you may be suffering from a condition known as adult acquired flat foot. As one of the main support structures of the foot?s arch, the tibilais posterior tendon, along with other muscles, tendons and ligaments, play a very important role in its mechanical function.
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.

Surgical Treatment
For more chronic flatfoot pain, surgical intervention may be the best option. Barring other serious medical ailments, surgery is a good alternative for patients with a serious problem. There are two surgical options depending on a person?s physical condition, age and lifestyle. The first type of surgery involves repair of the PTT by transferring of a nearby tendon to help re-establish an arch and straighten out the foot. After this surgery, patients wear a non-weight bearing support boot for four to six weeks. The other surgery involves fusing of two or three bones in the hind foot below the ankle. While providing significant pain relief, this option does take away some hind foot side-to-side motion. Following surgery, patients are in a cast for three months. Surgery is an effective treatment to address adult-acquired flatfoot, but it can sometimes be avoided if foot issues are resolved early. That is why it is so important to seek help right away if you are feeling ankle pain. But perhaps the best way to keep from becoming flatfooted is to avoid the risk factors altogether. This means keeping your blood pressure, weight and diabetes in check.
Have you noticed the arch in your foot collapse over a fairly short period of time as an adult? Or Do you suffer from pain on the inside and sole of your arch? If it does, then you may be suffering from a condition known as adult acquired flat foot. As one of the main support structures of the foot?s arch, the tibilais posterior tendon, along with other muscles, tendons and ligaments, play a very important role in its mechanical function.
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.
Surgical Treatment
For more chronic flatfoot pain, surgical intervention may be the best option. Barring other serious medical ailments, surgery is a good alternative for patients with a serious problem. There are two surgical options depending on a person?s physical condition, age and lifestyle. The first type of surgery involves repair of the PTT by transferring of a nearby tendon to help re-establish an arch and straighten out the foot. After this surgery, patients wear a non-weight bearing support boot for four to six weeks. The other surgery involves fusing of two or three bones in the hind foot below the ankle. While providing significant pain relief, this option does take away some hind foot side-to-side motion. Following surgery, patients are in a cast for three months. Surgery is an effective treatment to address adult-acquired flatfoot, but it can sometimes be avoided if foot issues are resolved early. That is why it is so important to seek help right away if you are feeling ankle pain. But perhaps the best way to keep from becoming flatfooted is to avoid the risk factors altogether. This means keeping your blood pressure, weight and diabetes in check.
Achilles Tendinitis Causes And Treatments
Overview
 A tendon is a tough yet flexible band of fibrous tissue. The tendon is the structure in your body that connects your muscles to the bones. The skeletal muscles in your body are responsible for moving your bones, thus enabling you to walk, jump, lift, and move in many ways. When a muscle contracts it pulls on a bone to cause movements. The structure that transmits the force of the muscle contraction to the bone is called a tendon. Tendons come in many shapes and sizes. Some are very small, like the ones that cause movements of your fingers, and some are much larger, such as your Achilles tendon in your heel. When functioning normally, these tendons glide easily and smoothly as the muscle contracts. Sometimes the tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal smooth gliding motion of your tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, and literally means inflammation of the tendon.
A tendon is a tough yet flexible band of fibrous tissue. The tendon is the structure in your body that connects your muscles to the bones. The skeletal muscles in your body are responsible for moving your bones, thus enabling you to walk, jump, lift, and move in many ways. When a muscle contracts it pulls on a bone to cause movements. The structure that transmits the force of the muscle contraction to the bone is called a tendon. Tendons come in many shapes and sizes. Some are very small, like the ones that cause movements of your fingers, and some are much larger, such as your Achilles tendon in your heel. When functioning normally, these tendons glide easily and smoothly as the muscle contracts. Sometimes the tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal smooth gliding motion of your tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, and literally means inflammation of the tendon.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
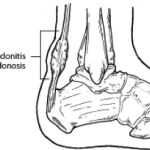
There is enlargement and warmth of the tendon 1 to 4 inches above its heel insertion. Pain and sometimes a scratching feeling may be created by gently squeezing the tendon between the thumb and forefinger during ankle motion. There may be weakness in push-off strength with walking. Magnetic resonance imaging (MRI) can define the extent of degeneration, the degree to which the tendon sheath is involved and the presence of other problems in this area, but the diagnosis is mostly clinical.
Nonsurgical Treatment
The recommended treatment for Achilles tendinitis consists of icing, gentle stretching, and modifying or limiting activity. Nonsteroidal anti-inflammatory medications (NSAIDs), such as ibuprofen or naprosyn, can reduce pain and swelling. Physical therapy and the use of an orthosis (heel lift) can also be helpful. For chronic cases where tendinosis is evident and other methods of treatment have failed, surgery may be recommended to remove and repair the damaged tissue.

Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
Regardless of whether the Achilles injury is insertional or non-insertional, a great method for lessening stress on the Achilles tendon is flexor digitorum longus exercises. This muscle, which originates along the back of the leg and attaches to the tips of the toes, lies deep to the Achilles. It works synergistically with the soleus muscle to decelerate the forward motion of the leg before the heel leaves the ground during propulsion. This significantly lessens strain on the Achilles tendon as it decelerates elongation of the tendon. Many foot surgeons are aware of the connection between flexor digitorum longus and the Achilles tendon-surgical lengthening of the Achilles (which is done to treat certain congenital problems) almost always results in developing hammer toes as flexor digitorum longus attempts to do the job of the recently lengthened tendon. Finally, avoid having cortisone injected into either the bursa or tendon-doing so weakens the tendon as it shifts production of collagen from type one to type three. In a recent study published in the Journal of Bone Joint Surgery(9), cortisone was shown to lower the stress necessary to rupture the Achilles tendon, and was particularly dangerous when done on both sides, as it produced a systemic effect that further weakened the tendon.
A tendon is a tough yet flexible band of fibrous tissue. The tendon is the structure in your body that connects your muscles to the bones. The skeletal muscles in your body are responsible for moving your bones, thus enabling you to walk, jump, lift, and move in many ways. When a muscle contracts it pulls on a bone to cause movements. The structure that transmits the force of the muscle contraction to the bone is called a tendon. Tendons come in many shapes and sizes. Some are very small, like the ones that cause movements of your fingers, and some are much larger, such as your Achilles tendon in your heel. When functioning normally, these tendons glide easily and smoothly as the muscle contracts. Sometimes the tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal smooth gliding motion of your tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, and literally means inflammation of the tendon.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
There is enlargement and warmth of the tendon 1 to 4 inches above its heel insertion. Pain and sometimes a scratching feeling may be created by gently squeezing the tendon between the thumb and forefinger during ankle motion. There may be weakness in push-off strength with walking. Magnetic resonance imaging (MRI) can define the extent of degeneration, the degree to which the tendon sheath is involved and the presence of other problems in this area, but the diagnosis is mostly clinical.
Nonsurgical Treatment
The recommended treatment for Achilles tendinitis consists of icing, gentle stretching, and modifying or limiting activity. Nonsteroidal anti-inflammatory medications (NSAIDs), such as ibuprofen or naprosyn, can reduce pain and swelling. Physical therapy and the use of an orthosis (heel lift) can also be helpful. For chronic cases where tendinosis is evident and other methods of treatment have failed, surgery may be recommended to remove and repair the damaged tissue.
Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
Regardless of whether the Achilles injury is insertional or non-insertional, a great method for lessening stress on the Achilles tendon is flexor digitorum longus exercises. This muscle, which originates along the back of the leg and attaches to the tips of the toes, lies deep to the Achilles. It works synergistically with the soleus muscle to decelerate the forward motion of the leg before the heel leaves the ground during propulsion. This significantly lessens strain on the Achilles tendon as it decelerates elongation of the tendon. Many foot surgeons are aware of the connection between flexor digitorum longus and the Achilles tendon-surgical lengthening of the Achilles (which is done to treat certain congenital problems) almost always results in developing hammer toes as flexor digitorum longus attempts to do the job of the recently lengthened tendon. Finally, avoid having cortisone injected into either the bursa or tendon-doing so weakens the tendon as it shifts production of collagen from type one to type three. In a recent study published in the Journal of Bone Joint Surgery(9), cortisone was shown to lower the stress necessary to rupture the Achilles tendon, and was particularly dangerous when done on both sides, as it produced a systemic effect that further weakened the tendon.